Meet Pedro, a 5-year-old warrior turning 6 this December. Pedro is one of three children in the Curiel family and is suffering from T Cell Acute Lymphoblastic leukemia (ALL). He is receiving delayed intensification treatments in California with his mom and siblings by his side.
“The past seven months have been the most aggressive chemo then he will go to maintenance where every other week he will receive chemo and eventually getting oral chemo which is not as intense,” his mom, Vilma notes. Vilma said that he’s had muscular stiffness from the new chemo which made him unable to walk and he did not want to get out of bed. “I think this is the most scary part of treatment. After 24 hours he started limping and getting back to his usual routine.”
When he’s not receiving treatment, he is found drawing treasure maps around the house. Vilma said that he loves to draw these maps and hide his “treasure” and have his two brothers go find it! He started homeschooling in August, and he can now read a full sentence. He is expected to return to school after flu season.
Pedro is currently in remission and maintenance will continue for the next three years.
FOR IMMEDIATE RELEASE – September 28, 2018 – Washington, D.C. – The American Childhood Cancer Organization (ACCO), the soleU.S. member of Childhood Cancer International (CCI) provided its overwhelming support today for the World Health Organization’s (WHO) announcement of its new global initiative to address the disparity between childhood cancer survival in low-middle versus high-income countries. The announcement came at the United Nations (UN) General Assembly’s side-meeting on childhood cancer which was organized by the Missions of the Republic of Uzbekistan, the Hashemite Kingdom of Jordan, El Salvador, the Republic of Moldova, the Kingdom of Morocco, the Republic of Philippines and the Russian Federation.
Funded through a generous donation from St. Jude Children’s Research Hospital, the WHO Global Initiative for Childhood Cancer partners with national and international *stakeholders including CCI to provide leadership and technical assistance to support governments in building and sustaining high-quality childhood cancer programs.
Each year, more than 300,000 children ages birth to 19 years are diagnosed with cancer around the world. Approximately 8 in 10 of these children live in low and middle-income countries where their survival rate is often near 20%. This is in stark contrast to high-income countries, where cure rates exceed 80% for many common childhood cancers.
How urgent is this global initiative? “Childhood cancer is the number one non-communicable disease (NCD) cause of death in children globally,” said Ruth Hoffman, ACCO’s Chief Executive Officer, and President of Childhood Cancer International. “Childhood cancer has no borders. Why should childhood cancer treatments and cures? Even in the U.S. the majority of children with cancer continue to be treated with old drugs that were developed in the 1950’s, ‘60’s and 70’s. These drugs cost very little yet are too often unavailable to the majority of children with cancer in the world who happen to live in low to middle income countries. With increased access to essential childhood cancer medicines and radiation, children can be cured of their disease regardless of where they live in the world.” Ms. Hoffman will continue to represent the voice of the families of children with cancer as a member of the WHO Global Initiative for Childhood Cancer.
Increase political commitment and capacity of countries to deliver best practices in childhood cancer diagnosis and treatment;
Support governments to develop high-quality cancer centers as well as develop standards and tools to guide the planning and implementation of interventions for early diagnosis, treatment and palliative and survivorship
care inclusive of the needs of childhood cancers;
Improve access to affordable essential child cancer medicines and technologies;
Support governments to safeguard families of children with cancer from social isolation and financial ruin as a result of cancer care;
Prioritize cancer as a child health priority and increase available funding at the national and global levels.
This initiative is founded on the World Health Assembly’s resolution Cancer Prevention and Control through an Integrated Approach (WHA70.12), which urges governments and WHO to accelerate action to achieve the targets specified in the Global Action Plan and 2030 UN Agenda for Sustainable Development to reduce premature mortality from cancer.
Actions to increase childhood cancer survival today represent effective and tangible steps as part of the broader fight against non-communicable diseases – steps that will catalyze global efforts to transform childhood cancer outcomes worldwide and ultimately save many more lives of children, now and for years to come.
*Some Stakeholders include: The International Society of Pediatric Oncology (SIOP), Intenational society of pediatric oncologists, Union for International Cancer Control (UICC), International Atomic Energy Agency (IAEA), International Agency for Research on Cancer (IARC), Sick Kids Hospital of Toronto, Texas Children’s Hospital, World Bank, Pediatric Oncology Rally to Transform Access to Global Essentials (PORTAGE), Friends of Cancer Patients (FOCP), Chai Clinton Health Access Initiative (CCHAI), BIO Ventures for Global Health (BVGH), Pharmaceutical Industry, International Federation of Pharmaceutical Manufacturers & Associations (IFPMA)
_________________________________
The American Childhood Cancer Organization was founded in Washington, D.C. in 1970 by parents of children and adolescents diagnosed with cancer to advocate for their needs and support research so every child survives and leads a long and healthy life. The U.S. largest grassroots organization at the forefront of the crucial battle against childhood cancer, the ACCO is dedicated to shaping policy, supporting research, raising awareness and providing educational resources and innovative programs to children with cancer, survivors and their families. Since its inception, the ACCO has helped support more than half a million families affected by childhood cancer. ACCO now has 35 local ACCO affiliates known as Founding Hope chapters throughout the United States. www.acco.org.
Childhood Cancer International (CCI) was founded in 1994 and is recognized as the largest patient support organization for childhood cancer in the world. Comprised of 188 member organizations in 98 countries, CCI represents the voice of children and adolescents with cancer, childhood cancer survivors and their families globally. Operating as a non-State Actor in official relations with the World Health Organization (WHO), CCI engages with the WHO as well as international develo
pment organizations, policy-makers, civil society organizations, research and medical professionals to advocate for the rights of children and adolescents with cancer and prioritize childhood cancer as an integral part of the local, national and global child health and development agenda.www.childhoodcancerinternational.org
FOR MORE INFORMATION OR TO SET UP AN INTERVIEW: Contact Ruth Hoffman, Chief Executive Officer, American Childhood Cancer Organization and President, Childhood Cancer International. rhoffman@acco.org; 202-262-9949.
Meet Beckham, one of our ambassadors for the month of September. He is a goofy 8 year old currently being treated for Stage 4 Neuroblastoma at Memorial Sloan Kettering in New York City. Beckham was diagnosed on September 11, 2013 at the age of 3. A few weeks prior to his diagnosis, Beckham was playing with his sister and they banged their heads together. This resulted in Beckham’s black eyes. His mom remembers looking at pictures from that time and seeing his eyes starting to darken.
“I called the doctor and they said to watch it and call if things worsened. They went down and then started to darken. I ended up taking him in to his pediatrician and they drew labs. Later that day I got a call that Beckham’s labs were abnormal and that we had an appointment with oncology up at Primary Children’s Hospital in Salt Lake City,” his mom recalls.
At first, doctors didn’t think Beckham had cancer, they went through many diagnoses, everything from mono to anemia. The doctors were not convinced and decided to do a bone marrow biopsy which revealed that Beckham had tumors throughout his body and bone marrow.
Treatment was aggressive and as a result Beckham started chemotherapy. The doctors performed a resection of the main tumor and radiation to his skull in Utah which resulted in soft tissue tumors and bone marrow clearing well but the tumors in his bones had hardly changed. Beckham’s mom recalls going onto a Facebook group for Neuroblastoma and was urged to take him for a second opinion at Memorial Sloan Kettering. February 2014 was the first trip to NYC where Beckham received MIBG therapy, NK cell therapy, radiation, 3f8 antibioties, cryotherapy surgery, numerous rounds of chemotherapy and surgery to remove lymph nodes in his upper right underarm and chest.
Beckham has had two central lines and is on his third port. “He has endured four relapses, the most recent being March of 2018 and his doctors say he is a miracle boy.”
Fortunately, his latest scans show no evidence of disease. He is currently in treatment for an alk mutation which was found in his past two surgeries. Beckham has a lot of personality and loves to make people laugh – we are looking forward to many laughs with Beckham!
Beckham is one strong little boy and an example of true perseverance. Beckham expresses to his mom that he is never giving up and his cancer is going down!
*Special thanks to our Candlelighters NYC Affiliate and Barbara Zobian*
Meet Braeden or “Brae” as his mom lovingly calls him. He’s a three year old, fun-loving “ladies man” who is wise beyond his years. Brae’s mom, Kendra noticed in January of 2018 that he was whining a lot. She took him to get checked out several times and after being told he had pneumonia, the flu and even being tested for having swallowed a toy, doctors decided to do a biopsy on his back. Doctors took a sample of the mass they found in his lungs and the diagnosis was clear. “On May 5, 2018, Brae was diagnosed with AML leukemia with a genetic mutation of monosomy 7. We just found out about the monosomy 7. Basically that means that Brae has 45 chromosomes instead of 46 like everyone else.”
Kendra was faced with a tough decision when it came to Brae’s treatment plan; get a bone marrow transplant and face three rounds of chemo with a 30% chance of relapse, or five rounds of chemo with a 60% chance of relapse. Kendra ultimately decided against the transplant and is happy to report that after Brae’s first round of chemo, his bulky tumor is gone. Doctors have continued to treat Brae with four more chemo rounds.
Fortunately, Braeden is facing treatment like a little soldier; the only side effect he has experienced was hair loss, which he doesn’t seem to mind. Kendra notes that everytime he goes into the hospital, the nurses fight to work with him and that he charms them. She said when Brae is at home, he loves to watch tv with his big brother and play outside. He’s particularly interested in art and loves to paint. When he goes to the hospital you can usually find him in the art room playing with the popsicle sticks and paint.
He mom happily informed us that he is currently ‘doing great’ after his fourth round of chemo. Through it all, Braeden is a positive and happy three year old.
There are nearly 5,000 new diagnoses of childhood leukemia every year in the United States, making this so-called “rare” disease the most common type of childhood cancer. In fact, childhood leukemia currently accounts for almost one-third of all childhood cancer diagnoses. Thanks to amazing advances in the efficacy of today’s treatment protocols, the majority of children diagnosed with leukemia today can expect to make a full recovery. The 5-year survival rates for the two main forms of leukemia—Acute lymphocytic (lymphoblastic) leukemia (ALL) and Acute myelogenous leukemia (AML)—are greater than 85% and about 60-70% respectively.
However, achieving remission and then joining the ranks of the “survivors” still requires that children undergo months, even years, of intensive chemotherapy. And despite the amazing advances in chemotherapy, it is still involves powerful drugs that can have serious and severe short- and long-term health risks. Indeed, one of the goals of researchers today is not only to ensure that no child dies of this dreaded disease, but also to find safer and less toxic treatment options. So while families are so focused on the short-term goal of survival, it is important to remain focused on both short- and long-term survivorship issues to help mitigate physical and emotional side effects.
Short Term Survivorship Issues
Perhaps the most critical step in monitoring and maintaining your child’s physical health during the first 2-5 years after treatment is ensuring that your child undergoes routine cancer screenings to watch for a relapse or recurrence of the cancer. These screenings are also useful for monitoring short- and long-term side effects of the chemotherapy. Although the schedule of screenings is different for each child, it usually consists of follow-up visits once a month or so for the first year after treatment, then decreasing in frequency after that. It is unusual for leukemia to return once a child has been cancer-free for 2 years or so, but most oncologists prefer to continue routine monitoring for at least five years.
While many parents are expecting concerns about their child’s physical health to predominate the immediate aftermath of treatment, most are surprised at the unexpected emotional and social issues that often arise after treatment. Challenges such as establishing a normal routine, going back to school, and reestablishing friendships and social connections often prove as difficult, or even more difficult, as the physical issues. Specific emotional issues vary depending on the age of the child and the duration of treatment, but luckily, most of these challenges are only temporary, and can be overcome with patience, encouragement, and lots of support from family, teachers, and even counsellors. Many cancer centers offer support services, in fact, to help families make this potentially difficult transition easier.
Long Term Survivorship Issues
In the long term, survivorship issues are usually focused on potential health concerns resulting from the toxicity of the chemotherapy treatments. Understanding the potential for long-term health problems is the first step to identifying and addressing these concerns as quickly as possible. The most common long-term health concerns among adult survivors of childhood leukemia include:
Secondary cancers: Chemotherapy has been linked to the development of other cancers in adulthood; for instance, treatment for ALL carries a small risk of developing AML as an adult.
Heart, lung, and bone problems: Some chemotherapy drugs can cause long-term damage to the heart and/or lungs, usually a higher risk for patients with ALL than AML. Steroid-based treatments have been linked to the development of osteoporosis.
Developmental delays/learning problems: Radiation therapy and some chemotherapy drugs have been linked to development delays in young children; therefore, most oncologists will try to avoid the use of radiation in young children whenever possible.
Growth delays: Some types of cancer treatments can impact a child’s natural growth.
Fertility concerns: Some chemotherapy drugs have been linked to problems related to sexual development and reproduction.
American Childhood Cancer Organization (ACCO) is a non-profit charity dedicated to helping kids with cancer and their families navigate the difficult journey from cancer diagnosis through survivorship. Internationally, ACCO is the sole U.S. member of Childhood Cancer International (CCI), the largest patient-support organization for childhood cancer in the world. Here in the United States, ACCO promotes the critical importance of ensuring continued funding into new and better treatment protocols for childhood cancer. And most importantly, ACCO is focused on the children: developing and providing educational tools for children fighting cancer and their families, empowering them in their understanding of childhood cancer and the medical decisions they must make during this difficult journey. All of ACCO’s resources are available free of charge for families coping with childhood cancer.
For additional information about childhood cancer or on the ACCO, or to order resources for you or your child, please visit our website at www.acco.org , call 855.858.2226 or visit:
Childhood leukemia is often pointed to as childhood cancer research’s success story. Just 60 years ago, almost no child with leukemia survived more than a few years, but today, thanks to new discoveries and advances in treatment, 90% of children with the most common type of leukemia will survive. That progress is certainly worth celebrating, but these statistics don’t tell the whole story. Let’s take a closer look at what these numbers really mean for children with leukemia.
What We Mean by “Survival”
When we talk about long-term survival for any childhood cancer, including leukemia, it is important to understand that oncologists and cancer researchers look at the five-year survival rate, or how many children remain cancer-free five years after the end of treatment. In general, children who are still cancer-free after five years are considered “cured” of the disease.
Thanks to advances in treatment methods, the five-year survival rate for childhood leukemia has greatly improved over the past several decades. The five-year survival rate for acute lymphoblastic leukemia (ALL) is now 90%. The five-year survival rate for acute myelogenous leukemia (AML) is lower, at 60-70%. Moreover, the rates can vary greatly depending on subtype and other factors.
These numbers do not, however, provide a specific prognosis for any given child. They are only averages compiled from treated cases of childhood leukemia across the country. Your child’s prognosis and long-term outlook after treatment will be heavily dependent on your child’s diagnosis, response to treatment, and general health.
Prognosis Factors for Childhood Leukemia
Prognosis factors are a series of measurements that your child’s oncology team may use to estimate the degree of risk posed by the cancer and to determine the most promising treatment plan. There are several key prognosis factors that oncologists use when dealing with a leukemia diagnosis. In general, these prognosis factors are the same for ALL and AML, but they do not seem to play as great a role in either guiding treatment or predicting outcomes for AML.
Risk group: A cancer can be classified as standard risk, high risk, or very high risk. These groupings help determine the intensity of treatment and may impact long-term prognosis.
Age at diagnosis: For B- cell ALL, children between the ages of 1 and 9 seem to have a more positive prognosis than children under the age of 1 or over the age of 10. Age does not appear to be a prognosis factor in T-cell ALL and AML.
Initial white blood cell count: Very high white blood cell counts at diagnosis is generally considered high risk or very high risk.
Subtype: There are many subtypes of leukemia, and some tend to be less aggressive and more responsive to treatment than others. For example, children diagnosed with pre-B, common, or early pre-B-cell ALL seem to have a more positive prognosis than children with mature B-cell leukemia, although B-cell ALL can also have a more positive prognosis if treated with intensive chemotherapy.
Gender: In general, girls seem to have a slightly better prognosis than boys, though this gap has shrunk in recent years thanks to today’s advanced treatment options.
Race/ethnicity: African-American and Hispanic children may have a slightly worse prognosis than other ethnicities.
Spread to other organs: If the leukemia has spread into the fluid around the brain and spinal cord, and the testicles in boys, it is usually classified as high-risk or very high-risk.
Number of chromosomes and chromosome translocations: Some studies have begun to link longer-term prognosis with the number of chromosomes within the leukemia cells, as well as with translocations between specific chromosomes (when part of a chromosome breaks off and attaches to another).
Response to treatment: The initial reduction of leukemia cells in the bone marrow during the first one to two weeks of chemotherapy may help determine long-term prognosis. If the leukemia does not respond as expected in this time frame, most oncologists will move to a more intensive treatment protocol.
Life for Childhood Leukemia Survivors
For several years after finishing treatment for leukemia, children will need to have regular exams to check for signs that the cancer has returned, as well as to monitor for side effects of treatment. Some side effects may appear during treatment or soon after the end, while others might not surface until adulthood.
While all childhood leukemia survivors have a greater risk of developing certain health problems as a result of their treatment, most side effects can be managed with proper medical care. It’s important that, even as adults, survivors continue to have regular health checks and are upfront with their healthcare providers about their cancer history.
Kaydence’s Story: Surviving ALL
Kaydence is no ordinary 7-year-old. She’s a talented budding artist with a penchant for donkeys, and she’s a survivor of acute lymphoblastic leukemia.
There was nothing ordinary about Kaydence’s cancer journey, either. She was found to have two rare chromosome mutations that classified her cancer as very high risk, and when she didn’t respond to the initial treatment, her parents and treatment team decided to move forward with CAR T-cell immunotherapy, a novel treatment that trains the patient’s own immune cells to target and kill the cancer cells.
It wasn’t an easy road. She spent 10 days on life support fighting septic shock two weeks after diagnosis. She went into anaphylactic shock after her T-cell infusion. She had to re-learn how to stand, walk, use her hands and fingers, and go to the toilet. But despite all the setbacks, Kaydence’s treatment was successful. She has been in remission since March 2019. Her immune system is still suppressed, so she has to take extra precautions to make sure she doesn’t get sick, and her doctors continue to monitor her closely for side effects or any signs of her cancer returning. But for her part, Kaydence is enjoying being her 7-year-old self: painting and crafting, playing with her siblings, and just being a normal kid.
September is Leukemia and Lymphoma Awareness Month. Help kids like Kaydence by making a donation to the American Childhood Cancer Organization to honor their fight during Leukemia Awareness Month. Your gift helps provide educational resources and support programs for children with cancer, survivors, and their families, as well as raise awareness about childhood cancer and the need for more research.
Together, we can make a difference.
Donate today… because kids can’t fight cancer alone®.
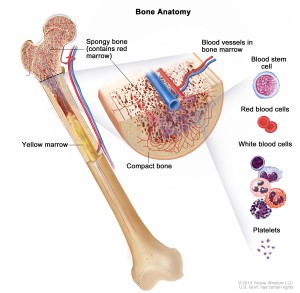
Both major types of childhood leukemia—Acute lymphocytic (lymphoblastic) leukemia (ALL) and Acute myelogenous leukemia (AML)—begin in the bone marrow, the soft inner part of the bone where new blood cells are created. As the leukemia cells accumulate inside the bone marrow, they overwhelm the healthy cells, eventually spreading into the blood stream. Thus, leukemia is a blood-based cancer, and must not be confused with other types of childhood cancers that start in other parts of the body and eventually spread into the bone marrow.
Why do some blood cells in children grow into abnormal leukemia cells? In other words, what causes childhood leukemia? Unfortunately, we cannot yet answer that question. We do know that childhood leukemia, like most other childhood cancers, is not caused by environmental or lifestyle factors. Absent these factors, scientists and researchers do not know what causes certain cells within a child’s bone marrow to begin growing and functioning abnormally.
Increasingly, scientists are beginning to believe that many childhood cancers, including leukemia, are linked to mutations—or random, uncontrolled alterations—to the DNA found within normal bone marrow cells. Leukemia may be connected to a specific type of DNA mutation controlling the genes responsible for ensuring that cells divide, grow, replicate, and die properly. Another potential cause of childhood leukemia may be a form of genetic mutation called chromosome translocation, where DNA from one chromosome breaks off and becomes attached to a different chromosome. Again, if this mutation affects oncogenes and/or tumor suppressor genes, it may lead to the development of childhood leukemia or other types of childhood cancer.
What are the risk factors for childhood leukemia?
If it is true that genetic mutations are responsible for most cases of childhood leukemia, it is important to note that these genetic mutations are usually the result of random and unpredictable changes and are not linked to any known or inherited risk. However, there are a few inherited conditions which may result in a higher risk factor for some rare cases of childhood leukemia, such as:
Inherited syndromes such as Down syndrome (trisomy 21) and Li-Fraumeni syndrome
Inherited immune system problems such as Ataxia-telangiectasia, Wiskott-Aldrich syndrome, Bloom syndrome, and Schwachman-Diamond syndrome
Having a sibling with leukemia, especially if the sibling is an identical twin
The one environmental factor that may pose an increased risk of childhood leukemia is exposure to extremely high levels of radiation (such as Japanese survivors of the 1945 atomic bombings). However, scientists are exploring any potential links between childhood leukemia and smaller dosages of radiation (like routine x-rays), as well as chemotherapy and exposure to toxic chemicals.
Can Childhood Leukemia Be Prevented?
Although we don’t yet know definitively what causes childhood cancer, we can say definitely that there is no way to prevent it, or as of right now, screen for it the way we can with many adult cancers. We can hope that as our understanding of the causes of leukemia and other childhood cancers improves, that knowledge brings with it a better understanding of how to detect the disease before it becomes the terrible threat that it poses today.
American Childhood Cancer Organization (ACCO) is a non-profit charity dedicated to helping kids with cancer and their families navigate the difficult journey from cancer diagnosis through survivorship. Internationally, ACCO is the sole U.S. member of Childhood Cancer International (CCI), the largest patient-support organization for childhood cancer in the world. Here in the United States, ACCO promotes the critical importance of ensuring continued funding into new and better treatment protocols for childhood cancer. And most importantly, ACCO is focused on the children: developing and providing educational tools for children fighting cancer and their families, empowering them in their understanding of childhood cancer and the medical decisions they must make during this difficult journey. All of ACCO’s resources are available free of charge for families coping with childhood cancer.
For additional information about childhood cancer or on the ACCO, or to order resources for you or your child, please visit our website at www.acco.org , call 855.858.2226 or visit:
Leukemia is the most common form of childhood cancer today, accounting for nearly one-third of all childhood cancer diagnoses in the United States. A blood-based cancer that begins in the soft inner part of the bone called the bone marrow, childhood leukemia is classified into three different types. The most common type is Acute lymphocytic (lymphoblastic) leukemia (ALL), about 75% of all childhood leukemia diagnoses. ALL starts with abnormal cell growth among immature lymphocytes (white blood cells that help the body fight infection). About 25% of diagnoses are Acute myelogenous leukemia (AML), which begins with abnormal growth of myeloid cells (responsible for the growth of non-lymphocytic white blood cells, red blood cells, and platelets.) The third type of childhood leukemia—Juvenile myelomonocytic leukemia (JMML)—is extremely rare. Like AML, it develops in the myeloid cells and is acute (quickly growing) but it does not develop and spread as quickly as either AML or ALL.
What are the Symptoms of Childhood Leukemia?
The signs and symptoms of childhood leukemia generally do not begin to manifest until the abnormal cancer cells have spread from inside the bone marrow into the blood stream. Once inside the blood stream, the leukemia cells begin to crowd out healthy blood cells, while simultaneously traveling throughout the body and impacting the health and normal functioning of other organs. Therefore, the specific signs and symptoms of leukemia depend on the type of blood cell has been most impacted by the growth of the abnormal cells, and the impact of the cancer on other organs throughout the body.
If leukemia has caused a shortage of healthy red blood cells, symptoms may include:
Fatigue
Weakness
Shortness of breath
Unusually pale skin
Headaches
An unusual sensation of cold
Lightheadedness or dizziness
If leukemia has caused a shortage of healthy white blood cells:
White blood cells are the body’s primary defense against illnesses caused by both bacteria and viruses. Therefore, if your child has a shortage of healthy white blood cells, or if the presence of leukemia cells is preventing the white blood cells from functioning properly, your child may not be able to fight off infections and illnesses. Recurring infections or infections that won’t go away even with medical intervention may indicate the presence of leukemia. The main indicator of infection is usually fever.
If leukemia has caused a shortage of platelets, signs and symptoms can include:
Easy and frequent bruising
Easy and frequent bleeding
Frequent and/or severe nosebleeds
Bleeding gums
If the leukemia has spread from the blood stream into or near other organs, it can cause symptoms relating to the functioning of those organs, such as:
Joint and/or bone pain
Swollen lymph nodes
Swelling in the abdomen
Weight loss and/or loss of appetite
Coughing or trouble breathing
Headaches, seizures, vomiting, loss of balance, and blurred vision
Swelling of the face and arms, called SVC syndrome, is a potentially very serious symptom caused by the accumulation of cancer cells in the thymus
Symptoms specific to AML include skin rashes, gum problems (swelling, pain, and bleeding), extreme weakness, extreme tiredness, and slurring of speech
With the exception of the serious symptoms such as SVC syndrome and the extreme fatigue and weakness seen (albeit rarely) in patients with AML, you may notice that the symptoms of childhood leukemia listed here are also symptoms of many routine childhood illnesses. The fact is that childhood leukemia is a very rare disease. Just because you notice the presence of one or more of these symptoms does not mean that your child has leukemia. However, if you have any concerns—and especially if you feel the symptoms are not going away or are getting worse—it is important to share your concerns with your child’s pediatrician. In some cases, he or she may suggest additional diagnostic testing if he or she believes that the symptoms may be related to childhood leukemia.
American Childhood Cancer Organization (ACCO) is a non-profit charity dedicated to helping kids with cancer and their families navigate the difficult journey from cancer diagnosis through survivorship. Internationally, ACCO is the sole U.S. member of Childhood Cancer International (CCI), the largest patient-support organization for childhood cancer in the world. Here in the United States, ACCO promotes the critical importance of ensuring continued funding into new and better treatment protocols for childhood cancer. And most importantly, ACCO is focused on the children: developing and providing educational tools for children fighting cancer and their families, empowering them in their understanding of childhood cancer and the medical decisions they must make during this difficult journey. All of ACCO’s resources are available free of charge for families coping with childhood cancer.
For additional information about childhood cancer or on the ACCO, or to order resources for you or your child, please visit our website at www.acco.org , call 855.858.2226 or visit:
Treatment for neuroblastoma can be long, difficult, and traumatic, not only for the patient but also for friends and family. Once treatment has ended and your child has been declared “cancer free”, it is very common for everyone—patient and family alike—to look forward to returning to “normal life.” And for the most part, it is possible to get back to a life that doesn’t revolve around childhood cancer. At the same time, however, it is important to recognize that childhood cancer has both short- and long-term consequences—both physical and emotional—that can continue to impact your child’s return to cancer-free normalcy.
Experts agree that the first step in facing life as a neuroblastoma survivor is working with your child’s oncology team to develop a comprehensive survivorship care plan. Such a plan can act as a checklist to help you ensure your child’s short- and long-term health, both physical and emotional, as well as smooth the transition back into a normal cancer-free life. Although the basic outline of any survivorship care plan is fairly standard, your child’s specific plan will be unique to him or her, depending on the characteristics of your child’s cancer and its treatment, as well as your child’s general health.
Your Child’s Survivorship Care Plan
Follow-up exams and tests
One of the most common concerns among parents and families of childhood cancer survivors is, will the cancer return? As of right now, scientists do not believe that there are any steps a parent or child can do after treatment has concluded to reduce the potential for recurrence. Parents can, however, develop—and then stick to—a scheduled plan of follow-up tests and scans. Depending on your child’s risk grouping, size and location of the original tumor, and other factors, tests will probably include both lab work and imaging tests such as PET scans, CT scans, and/or MRIs. As time goes on without recurrence, the time between tests will increase, and eventually the focus may switch to early detection screenings that focus on long-term health effects and/or secondary cancers.
Maintain complete and accurate medical records
As your child begins life as a childhood cancer survivor, it is important to remember that neuroblastoma will impact your child’s life for years to come. Therefore, it is critical to maintain accurate and complete medical records of your child’s entire cancer journey, from first diagnosis through treatment and including post-treatment screenings. Should your child experience health concerns later in life, future physicians will need to know this part of your child’s medical history in detail in order to develop a correct and comprehensive treatment plan.
Possible short- and long-term health effects of neuroblastoma and its treatment
Neuroblastoma and its treatment can, unfortunately, have long-term health effects, often called “late effects.” These may stem from the cancer itself, or from the treatment required to fight the neuroblastoma. Some late effects may present during or immediately after treatment; some may not begin until years later. Some of the most common late effects of neuroblastoma include:
Hearing loss
Bone and/or musculature problems (such as scoliosis)
Thyroid problems
Growth and development concerns
Fertility problems
Neurological concerns
Secondary cancers
Opsoclonus myoclonus syndrome (a very rare syndrome in which the body’s immune system begins to attack normal nerve tissue, causing learning disabilities, delayed muscle development, language delays, and behavioral problems)
Problems with the eyes or with muscle twitches (common in children with tumors located in the neck or chest, may require further treatment with corticosteroids or IVIG)
Emotional and social concerns
In the eagerness to return to “normalcy”, it can be all-too-easy to overlook the emotional stress that childhood cancer puts on both the child and his or her family, emotional stress that can continue to linger once treatment is complete. For older children, returning to school and social activities can prove more challenging than many families anticipate. Many cancer treatment centers can provide access to social workers and counsellors who can help families recognize and cope with the emotional strain of childhood cancer and its treatment.
American Childhood Cancer Organization (ACCO) is a non-profit charity dedicated to helping kids with cancer and their families navigate the difficult journey from cancer diagnosis through survivorship. Internationally, ACCO is the sole U.S. member of Childhood Cancer International (CCI), the largest patient-support organization for childhood cancer in the world. Here in the United States, ACCO promotes the critical importance of ensuring continued funding into new and better treatment protocols for childhood cancer. And most importantly, ACCO is focused on the children: developing and providing educational tools for children fighting cancer and their families, empowering them in their understanding of childhood cancer and the medical decisions they must make during this difficult journey. All of ACCO’s resources are available free of charge for families coping with childhood cancer.
For additional information about childhood cancer or on the ACCO, or to order resources for you or your child, please visit our website at www.acco.org , call 855.858.2226 or visit:
Nearly one-third of all children and teens with cancer are diagnosed with childhood leukemia, making this form of childhood cancer by far the most common. Childhood leukemia is a cancer of the blood. It begins in the bone marrow, the soft interior of the bones responsible for the development of new blood cells. Leukemia cells in the bone marrow replicate more quickly than healthy cells, and do not die at the proper time, and eventually begin to crowd out healthy cells. As this happens, the cancerous cells enter the blood stream and quickly move around the body. As the leukemia cells invade other organs, they begin to impact the ability of those organs to function normally.
There are two main types of acute childhood leukemia: ALL and AML:
Acute lymphocytic (lymphoblastic) leukemia (ALL): ALL is the most common form of childhood leukemia, accounting for approximately 75% of leukemia diagnoses. ALL develops from immature lymphocytes, which when healthy grow into white blood cells responsible for fighting infections and bacteria. Most ALL cases involve B cells, the lymphocytes responsible for making the antibodies that the body uses to fight viruses; however, some cases of ALL originate in T cells, which are responsible for fighting infection themselves.
Acute myelogenous leukemia (AML): Approximately 25% of childhood leukemia cases are AML, also known as acute myeloid leukemia, acute myelocytic leukemia, or acute non-lymphocytic leukemia. AML originates in myeloid cells that are responsible for developing non-lymphocytic white blood cells, red blood cells, and platelets.
Juvenile myelomonocytic leukemia (JMML) is a very rare type of childhood leukemia that is usually diagnosed in children under the age of 4. Like AML, it originates in myeloid cells, but develops much more slowly than AML (yet still grows more rapidly than chronic leukemia common in adults). Chronic (slow-growing) leukemias such as chronic myelogenous leukemia (CML) and chronic lymphocytic leukemia (CLL) are extremely rare in children.
Detection and Diagnosis of Childhood Leukemia
Children are usually diagnosed with childhood leukemia once it has entered the blood stream and spread to other parts of the body, leading to visible symptoms of illness as the leukemia cells prevent the normal functioning of various organs. The most common symptoms of childhood leukemia are fatigue, headaches, paleness, fever, and infection. Of course, these are similar to symptoms of many routine childhood ailments; however, your child’s pediatrician may recognize them as potential warning signs of leukemia if they persist, reoccur frequently, and/or gradually worsen over time despite treatment. Easy bruising and bleeding is also a potential symptom of leukemia.
Should your child’s pediatrician believe that leukemia may be the source of your child’s symptoms, he or she will recommend a blood test, which can indicate the potential presence of leukemia cells in the blood. The blood test will determine how many cells of each type (red blood cells, white blood cells, and platelets) are present in your child’s blood. An abnormally high level of white blood cells and a corresponding low level of red blood cells and platelets may indicate leukemia. A technician will also examine the blood sample under a microscope to look for abnormalities in the blood cells themselves.
Should this blood test indicate the potential presence of leukemia in your child’s blood stream, your child will be referred to an oncologist for full diagnostic testing. The first step in a leukemia diagnosis is a bone marrow aspiration and biopsy. This test is done to determine if leukemia cells are present in the bone marrow itself. Usually performed together, a bone marrow aspiration involves removing a small amount of bone marrow through a syringe inserted through the bone via a thin, hollow needle. Then, using a slightly larger needle, a small piece of the bone together with some marrow is removed. The biopsy involves examining the bone and the marrow samples under a microscope to detect the presence of leukemia cells.
If your child is diagnosed with leukemia, his or her oncology team will begin a series of additional tests and scans in order to classify and stage the leukemia. These tests will help the oncologists determine the appropriate method of treatment. These additional tests may include:
Lumbar puncture (otherwise known as a spinal tap) in order to determine if there are leukemia cells in the cerebrospinal fluid
Chest x-ray: to detect the potential for an enlarged thymus or lymph nodes, as well as to determine if there is any pneumonia and/or lung infection
CT scan or MRI: to detect the presence of leukemia in other organs such as the lymph nodes, spleen, liver, brain, and/or spinal cord
PET scan: may be helpful in determining the extent to which leukemia cells have spread throughout the body
American Childhood Cancer Organization (ACCO) is a non-profit charity dedicated to helping kids with cancer and their families navigate the difficult journey from cancer diagnosis through survivorship. Internationally, ACCO is the sole U.S. member of Childhood Cancer International (CCI), the largest patient-support organization for childhood cancer in the world. Here in the United States, ACCO promotes the critical importance of ensuring continued funding into new and better treatment protocols for childhood cancer. And most importantly, ACCO is focused on the children: developing and providing educational tools for children fighting cancer and their families, empowering them in their understanding of childhood cancer and the medical decisions they must make during this difficult journey. All of ACCO’s resources are available free of charge for families coping with childhood cancer.
For additional information about childhood cancer or on ACCO, or to order resources for you or your child, please visit our website at www.acco.org.
For additional information about childhood cancer or on the ACCO, or to order resources for you or your child, please visit our website at www.acco.org , call 855.858.2226 or visit:



 Meet Pedro, a 5-year-old warrior turning 6 this December. Pedro is one of three children in the Curiel family and is suffering from T Cell Acute Lymphoblastic leukemia (ALL). He is receiving delayed intensification treatments in California with his mom and siblings by his side.
Meet Pedro, a 5-year-old warrior turning 6 this December. Pedro is one of three children in the Curiel family and is suffering from T Cell Acute Lymphoblastic leukemia (ALL). He is receiving delayed intensification treatments in California with his mom and siblings by his side. 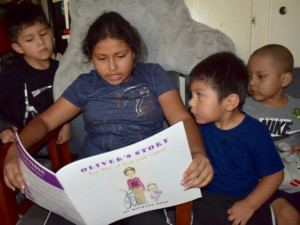 When he’s not receiving treatment, he is found drawing treasure maps around the house. Vilma said that he loves to draw these maps and hide his “treasure” and have his two brothers go find it! He started homeschooling in August, and he can now read a full sentence. He is expected to return to school after flu season.
When he’s not receiving treatment, he is found drawing treasure maps around the house. Vilma said that he loves to draw these maps and hide his “treasure” and have his two brothers go find it! He started homeschooling in August, and he can now read a full sentence. He is expected to return to school after flu season.  announcement of its new global initiative to address the disparity between childhood cancer survival in low-middle versus high-income countries. The announcement came at the United Nations (UN) General Assembly’s side-meeting on childhood cancer
announcement of its new global initiative to address the disparity between childhood cancer survival in low-middle versus high-income countries. The announcement came at the United Nations (UN) General Assembly’s side-meeting on childhood cancer 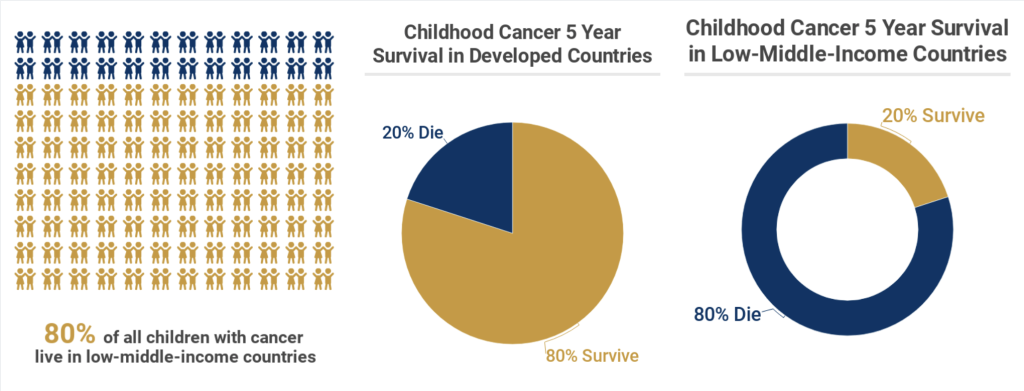
 Meet Beckham, one of our ambassadors for the month of September. He is a goofy 8 year old currently being treated for Stage 4 Neuroblastoma at Memorial Sloan Kettering in New York City. Beckham was diagnosed on September 11, 2013 at the age of 3. A few weeks prior to his diagnosis, Beckham was playing with his sister and they banged their heads together. This resulted in Beckham’s black eyes. His mom remembers looking at pictures from that time and seeing his eyes starting to darken.
Meet Beckham, one of our ambassadors for the month of September. He is a goofy 8 year old currently being treated for Stage 4 Neuroblastoma at Memorial Sloan Kettering in New York City. Beckham was diagnosed on September 11, 2013 at the age of 3. A few weeks prior to his diagnosis, Beckham was playing with his sister and they banged their heads together. This resulted in Beckham’s black eyes. His mom remembers looking at pictures from that time and seeing his eyes starting to darken.  At first, doctors didn’t think Beckham had cancer, they went through many diagnoses, everything from mono to anemia. The doctors were not convinced and decided to do a bone marrow biopsy which revealed that Beckham had tumors throughout his body and bone marrow.
At first, doctors didn’t think Beckham had cancer, they went through many diagnoses, everything from mono to anemia. The doctors were not convinced and decided to do a bone marrow biopsy which revealed that Beckham had tumors throughout his body and bone marrow.  Treatment was aggressive and as a result Beckham started chemotherapy. The doctors performed a resection of the main tumor and radiation to his skull in Utah which resulted in soft tissue tumors and bone marrow clearing well but the tumors in his bones had hardly changed. Beckham’s mom recalls going onto a Facebook group for Neuroblastoma and was urged to take him for a second opinion at Memorial Sloan Kettering. February 2014 was the first trip to NYC where Beckham received MIBG therapy, NK cell therapy, radiation, 3f8 antibioties, cryotherapy surgery, numerous rounds of chemotherapy and surgery to remove lymph nodes in his upper right underarm and chest.
Treatment was aggressive and as a result Beckham started chemotherapy. The doctors performed a resection of the main tumor and radiation to his skull in Utah which resulted in soft tissue tumors and bone marrow clearing well but the tumors in his bones had hardly changed. Beckham’s mom recalls going onto a Facebook group for Neuroblastoma and was urged to take him for a second opinion at Memorial Sloan Kettering. February 2014 was the first trip to NYC where Beckham received MIBG therapy, NK cell therapy, radiation, 3f8 antibioties, cryotherapy surgery, numerous rounds of chemotherapy and surgery to remove lymph nodes in his upper right underarm and chest.  Beckham has had two central lines and is on his third port. “He has endured four relapses, the most recent being March of 2018 and his doctors say he is a miracle boy.”
Beckham has had two central lines and is on his third port. “He has endured four relapses, the most recent being March of 2018 and his doctors say he is a miracle boy.” 


 Fortunately, Braeden is facing treatment like a little soldier; the only side effect he has experienced was hair loss, which he doesn’t seem to mind. Kendra notes that everytime he goes into the hospital, the nurses fight to work with him and that he charms them. She said when Brae is at home, he loves to watch tv with his big brother and play outside. He’s particularly interested in art and loves to paint. When he goes to the hospital you can usually find him in the art room playing with the popsicle sticks and paint.
Fortunately, Braeden is facing treatment like a little soldier; the only side effect he has experienced was hair loss, which he doesn’t seem to mind. Kendra notes that everytime he goes into the hospital, the nurses fight to work with him and that he charms them. She said when Brae is at home, he loves to watch tv with his big brother and play outside. He’s particularly interested in art and loves to paint. When he goes to the hospital you can usually find him in the art room playing with the popsicle sticks and paint.  There are nearly 5,000 new diagnoses of childhood leukemia every year in the United States, making this so-called “rare” disease the most common type of childhood cancer. In fact, childhood leukemia currently accounts for almost one-third of all childhood cancer diagnoses. Thanks to amazing advances in the efficacy of today’s treatment protocols, the majority of children diagnosed with leukemia today can expect to make a full recovery. The 5-year survival rates for the two main forms of leukemia—Acute lymphocytic (lymphoblastic) leukemia (ALL) and Acute myelogenous leukemia (AML)—are greater than 85% and about 60-70% respectively.
There are nearly 5,000 new diagnoses of childhood leukemia every year in the United States, making this so-called “rare” disease the most common type of childhood cancer. In fact, childhood leukemia currently accounts for almost one-third of all childhood cancer diagnoses. Thanks to amazing advances in the efficacy of today’s treatment protocols, the majority of children diagnosed with leukemia today can expect to make a full recovery. The 5-year survival rates for the two main forms of leukemia—Acute lymphocytic (lymphoblastic) leukemia (ALL) and Acute myelogenous leukemia (AML)—are greater than 85% and about 60-70% respectively.

 Both major types of childhood leukemia—Acute lymphocytic (lymphoblastic) leukemia (ALL) and Acute myelogenous leukemia (AML)—begin in the bone marrow, the soft inner part of the bone where new blood cells are created. As the leukemia cells accumulate inside the bone marrow, they overwhelm the healthy cells, eventually spreading into the blood stream. Thus, leukemia is a blood-based cancer, and must not be confused with other types of childhood cancers that start in other parts of the body and eventually spread into the bone marrow.
Both major types of childhood leukemia—Acute lymphocytic (lymphoblastic) leukemia (ALL) and Acute myelogenous leukemia (AML)—begin in the bone marrow, the soft inner part of the bone where new blood cells are created. As the leukemia cells accumulate inside the bone marrow, they overwhelm the healthy cells, eventually spreading into the blood stream. Thus, leukemia is a blood-based cancer, and must not be confused with other types of childhood cancers that start in other parts of the body and eventually spread into the bone marrow. Leukemia is the most common form of childhood cancer today, accounting for nearly one-third of all childhood cancer diagnoses in the United States. A blood-based cancer that begins in the soft inner part of the bone called the bone marrow, childhood leukemia is classified into three different types. The most common type is Acute lymphocytic (lymphoblastic) leukemia (ALL), about 75% of all childhood leukemia diagnoses. ALL starts with abnormal cell growth among immature lymphocytes (white blood cells that help the body fight infection). About 25% of diagnoses are Acute myelogenous leukemia (AML), which begins with abnormal growth of myeloid cells (responsible for the growth of non-lymphocytic white blood cells, red blood cells, and platelets.) The third type of childhood leukemia—Juvenile myelomonocytic leukemia (JMML)—is extremely rare. Like AML, it develops in the myeloid cells and is acute (quickly growing) but it does not develop and spread as quickly as either AML or ALL.
Leukemia is the most common form of childhood cancer today, accounting for nearly one-third of all childhood cancer diagnoses in the United States. A blood-based cancer that begins in the soft inner part of the bone called the bone marrow, childhood leukemia is classified into three different types. The most common type is Acute lymphocytic (lymphoblastic) leukemia (ALL), about 75% of all childhood leukemia diagnoses. ALL starts with abnormal cell growth among immature lymphocytes (white blood cells that help the body fight infection). About 25% of diagnoses are Acute myelogenous leukemia (AML), which begins with abnormal growth of myeloid cells (responsible for the growth of non-lymphocytic white blood cells, red blood cells, and platelets.) The third type of childhood leukemia—Juvenile myelomonocytic leukemia (JMML)—is extremely rare. Like AML, it develops in the myeloid cells and is acute (quickly growing) but it does not develop and spread as quickly as either AML or ALL. Treatment for neuroblastoma can be long, difficult, and traumatic, not only for the patient but also for friends and family. Once treatment has ended and your child has been declared “cancer free”, it is very common for everyone—patient and family alike—to look forward to returning to “normal life.” And for the most part, it is possible to get back to a life that doesn’t revolve around childhood cancer. At the same time, however, it is important to recognize that childhood cancer has both short- and long-term consequences—both physical and emotional—that can continue to impact your child’s return to cancer-free normalcy.
Treatment for neuroblastoma can be long, difficult, and traumatic, not only for the patient but also for friends and family. Once treatment has ended and your child has been declared “cancer free”, it is very common for everyone—patient and family alike—to look forward to returning to “normal life.” And for the most part, it is possible to get back to a life that doesn’t revolve around childhood cancer. At the same time, however, it is important to recognize that childhood cancer has both short- and long-term consequences—both physical and emotional—that can continue to impact your child’s return to cancer-free normalcy. Nearly one-third of all children and teens with cancer are diagnosed with childhood leukemia, making this form of childhood cancer by far the most common. Childhood leukemia is a cancer of the blood. It begins in the bone marrow, the soft interior of the bones responsible for the development of new blood cells. Leukemia cells in the bone marrow replicate more quickly than healthy cells, and do not die at the proper time, and eventually begin to crowd out healthy cells. As this happens, the cancerous cells enter the blood stream and quickly move around the body. As the leukemia cells invade other organs, they begin to impact the ability of those organs to function normally.
Nearly one-third of all children and teens with cancer are diagnosed with childhood leukemia, making this form of childhood cancer by far the most common. Childhood leukemia is a cancer of the blood. It begins in the bone marrow, the soft interior of the bones responsible for the development of new blood cells. Leukemia cells in the bone marrow replicate more quickly than healthy cells, and do not die at the proper time, and eventually begin to crowd out healthy cells. As this happens, the cancerous cells enter the blood stream and quickly move around the body. As the leukemia cells invade other organs, they begin to impact the ability of those organs to function normally.