


 Meet courageous Colton Whisler, a four-year-old warrior currently battling Perimeningeal Rhabdomyosarcoma, otherwise known as RMS. We were pleased to connect with Colton’s family through The Mark White Show, a popular radio program in Alabama.
Meet courageous Colton Whisler, a four-year-old warrior currently battling Perimeningeal Rhabdomyosarcoma, otherwise known as RMS. We were pleased to connect with Colton’s family through The Mark White Show, a popular radio program in Alabama.
In October 2018, Colton had experienced a facial droop that was originally diagnosed as Bell’s Palsy. Stephanie Whisler, Colton’s mom said “ we were told it was harmless and it would go away. He began crying and saying his ear was hurting. He then told us the floor was spinning.” At this point, Stephanie knew something was wrong with Colton. She decided to take him to his pediatrician at least once a week for the next three weeks where they treated him for a bad ear infection. Colton was then referred to an ear, nose and throat doctor (ENT) for tubes but when the pediatrician called him, the ENT thought it was something more. The ENT ended up meeting the Whisler family on his day off and found out that it wasn’t just an ear infection, it was a tumor. “We were in a state of shock, it was so hard to believe that our sweet perfect baby would be beginning the fight for his life,” said Stephanie.
Colton will be receiving approximately 15 months of chemo and radiation treatment and 30 treatments of proton therapy. According to his mom, “his age is both a blessing and a curse. He is young enough that he doesn’t really understand the severity of his situation, but he also can’t verbalize what he is feeling. Being away from his big brother, Ty, has been one of the hardest parts of this for both of them.” Since Colton’s tumor is in the middle of the ear, it is considered inoperable. The Whisler’s have discussed end of treatment surgeries consisting of a cochlear implant and surgery to correct his facial droop.
Chemotherapy hasn’t been easy for Colton either. His mom told ACCO, “his journey started off really rough. The first round was incredibly hard on him. The amazing doctors and nurses have since come up with a strategy that helps to keep his nausea at bay.”
Colton is currently in the hospital receiving treatment. He is experiencing neuropathy of his feet due to a weekly drug he takes. He is in physical therapy twice a week and will be receiving braces for his legs soon. According to Colton, “courageous people never give up and nothing is going to steal my joy.’’










For more about Courageous Colton Whisler: https://www.facebook.com/Courageous-Coltons-Crew
For more information about Permeningeal Rhabdomyosarcoma please visit: https://www.acco.org/sarcomas/
We can help! For free resources please visit: https://www.tfaforms.com/4699752
Together, we can make a difference.
Donate today because kids can’t fight cancer alone®.

About American Childhood Cancer Organization
The American Childhood Cancer Organization was founded in 1970 by parents of children and adolescents diagnosed with cancer. As the nation’s oldest and largest grassroots organization dedicated to childhood cancer, ACCO is committed to shaping policy, supporting research, raising awareness, and providing free educational resources to kids with cancer, survivors, and their families. Additionally, ACCO is the sole U.S. member of Childhood Cancer International (CCI) and has helped support more than half a million families over the past 50 years. Help make childhood cancer a national health priority because kids can’t fight cancer alone®.
For more information about how ACCO can help your family, call 855.858.2226 or visit:
 The brain and the spinal cord make up what is known as the Central Nervous System (CNS) and together, they control nearly all of our body’s normal functions. The brain is composed of three major parts.
The brain and the spinal cord make up what is known as the Central Nervous System (CNS) and together, they control nearly all of our body’s normal functions. The brain is composed of three major parts.
 Baseball season started in March of 2018 and Damon came home one day after practice saying that his right knee felt like his left one previously. They didn’t really think anything of it – so Damon finished out the baseball season the best he could. Damon’s mother, Tiffiney said, “for a minute the world stopped and went dark. It was Damon’s 16th birthday. It was something that we were somewhat prepared for thanks in part to our spor
Baseball season started in March of 2018 and Damon came home one day after practice saying that his right knee felt like his left one previously. They didn’t really think anything of it – so Damon finished out the baseball season the best he could. Damon’s mother, Tiffiney said, “for a minute the world stopped and went dark. It was Damon’s 16th birthday. It was something that we were somewhat prepared for thanks in part to our spor


 The central nervous system—including the brain and the spinal cord—grows and develops very quickly during childhood. This rapid rate of growth and development can make treating a brain and/or spinal cord tumor in children especially complicated for several reasons. First, the growth of the tumor can more easily damage the rapidly-changing tissues of the central nervous system (CNS). Second, the tissues of the CNS are extremely sensitive to the potentially damaging impact of chemotherapy, radiation, and other tools required to eliminate the tumor. These two issues are especially concerning when discussing survivorship issues for childhood brain and spinal cord tumors, and may have repercussions well into adulthood.
The central nervous system—including the brain and the spinal cord—grows and develops very quickly during childhood. This rapid rate of growth and development can make treating a brain and/or spinal cord tumor in children especially complicated for several reasons. First, the growth of the tumor can more easily damage the rapidly-changing tissues of the central nervous system (CNS). Second, the tissues of the CNS are extremely sensitive to the potentially damaging impact of chemotherapy, radiation, and other tools required to eliminate the tumor. These two issues are especially concerning when discussing survivorship issues for childhood brain and spinal cord tumors, and may have repercussions well into adulthood.
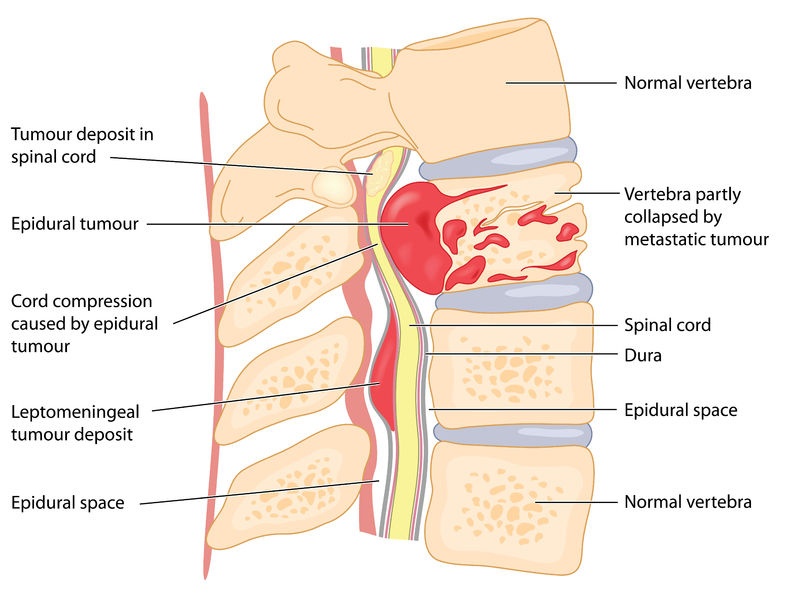
 By August, Kirby was completely paralyzed from the waist down. The doctors wouldn’t listen. Kirby’s parents decided to take matters into their own hands and took Kirby to a larger hospital to go through more tests. After a tearful meeting with one doctor expressing she didn’t know what was wrong with Kirby, they ordered an MRI. Moments after the MRI was read, the doctor told Sonnie, “we found out what is wrong with your son, he has tumors on his spine and they are spreading. It’s cancer. We need to get him on an airplane on our way to Children’s Hospital.” By noon, the family was on an airplane to Children’s Hospital of Colorado – a home to the Sargent family for the next six months.
By August, Kirby was completely paralyzed from the waist down. The doctors wouldn’t listen. Kirby’s parents decided to take matters into their own hands and took Kirby to a larger hospital to go through more tests. After a tearful meeting with one doctor expressing she didn’t know what was wrong with Kirby, they ordered an MRI. Moments after the MRI was read, the doctor told Sonnie, “we found out what is wrong with your son, he has tumors on his spine and they are spreading. It’s cancer. We need to get him on an airplane on our way to Children’s Hospital.” By noon, the family was on an airplane to Children’s Hospital of Colorado – a home to the Sargent family for the next six months.

 What are the key prognosis factors for childhood brain tumors?
What are the key prognosis factors for childhood brain tumors? When classed together in a single grouping, cancers in the brain and spinal cord are the second most common type of childhood cancer after leukemia. Brain and spinal cord tumors account for about 25% of all childhood cancer diagnoses, with more than 4,000 new cases diagnosed every year in the United States. In reality, however, it can be difficult to discuss “brain tumors” in general terms: oncologists recognize at least nine different sub-classifications of brain tumors in children, such as brain stem gliomas and ependymomas for example, with still more sub-groupings within those broad classifications.
When classed together in a single grouping, cancers in the brain and spinal cord are the second most common type of childhood cancer after leukemia. Brain and spinal cord tumors account for about 25% of all childhood cancer diagnoses, with more than 4,000 new cases diagnosed every year in the United States. In reality, however, it can be difficult to discuss “brain tumors” in general terms: oncologists recognize at least nine different sub-classifications of brain tumors in children, such as brain stem gliomas and ependymomas for example, with still more sub-groupings within those broad classifications.

 Grace loves to be crafty; she made a sign for the children to sign and date which says “Last Day of Chemo.” Throughout her treatment, she decided to paint pictures to brighten the nurses and the children’s days. When losing her hair became a reality, Grace decided to throw a party and shave her head. Grace’s brother and her best friend joined her in shaving their heads as well.
Grace loves to be crafty; she made a sign for the children to sign and date which says “Last Day of Chemo.” Throughout her treatment, she decided to paint pictures to brighten the nurses and the children’s days. When losing her hair became a reality, Grace decided to throw a party and shave her head. Grace’s brother and her best friend joined her in shaving their heads as well. lking to people about this part of her journey and is focused on helping others. Grace plans on learning more about oncology. She is excited for the future and can’t wait for her hair to start growing back!
lking to people about this part of her journey and is focused on helping others. Grace plans on learning more about oncology. She is excited for the future and can’t wait for her hair to start growing back! 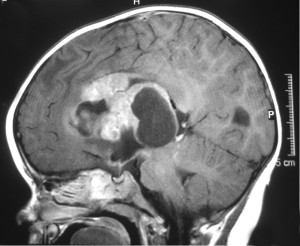 Any time a child is diagnosed with a brain tumor or other type of cancer, the most obvious question many parents ask is “why”. What caused this child to develop a brain tumor? Unfortunately, there is no easy answer to this question. Scientists now believe that the vast majority of brain tumors in children are the result of random gene mutations but have no satisfying answer as to why a particular gene mutation occurred or why it led to the growth of a brain tumor.
Any time a child is diagnosed with a brain tumor or other type of cancer, the most obvious question many parents ask is “why”. What caused this child to develop a brain tumor? Unfortunately, there is no easy answer to this question. Scientists now believe that the vast majority of brain tumors in children are the result of random gene mutations but have no satisfying answer as to why a particular gene mutation occurred or why it led to the growth of a brain tumor. After leukemia, brain tumors (including spinal cord tumors) are the second-most common type of cancer in children, accounting for about 25% of all childhood cancer diagnoses. Brain tumors begin within the delicate and complicated tissues of the brain or the cerebrospinal fluid (as well as the spinal cord or central nervous system, as these tumors are usually classed with brain tumors in children). When dealing with brain tumors in children, oncologists rarely differentiate between benign (non-cancerous) or malignant (cancerous) tumors; all tumors in the brain can be life-threatening whether technically cancerous or not. Instead, oncologists usually focus on how fast the tumor is growing, how quickly or easily it may spread throughout the brain or spinal cord, and how easy the tumor is to remove completely.
After leukemia, brain tumors (including spinal cord tumors) are the second-most common type of cancer in children, accounting for about 25% of all childhood cancer diagnoses. Brain tumors begin within the delicate and complicated tissues of the brain or the cerebrospinal fluid (as well as the spinal cord or central nervous system, as these tumors are usually classed with brain tumors in children). When dealing with brain tumors in children, oncologists rarely differentiate between benign (non-cancerous) or malignant (cancerous) tumors; all tumors in the brain can be life-threatening whether technically cancerous or not. Instead, oncologists usually focus on how fast the tumor is growing, how quickly or easily it may spread throughout the brain or spinal cord, and how easy the tumor is to remove completely.