

Meet the Rush family warriors: Tristen, 6, Caison, 3, and Carter, 8 months old. Each of the boys have bravely fought retinoblastoma at a very young age. 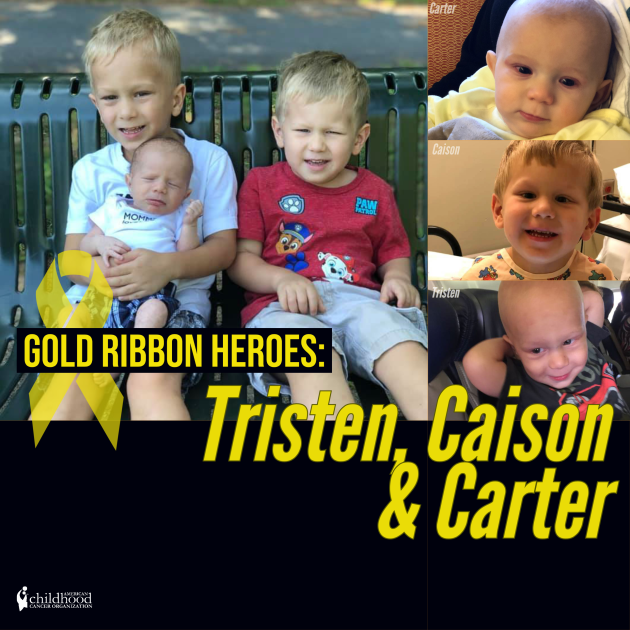
When Angie Rush was an infant, she was diagnosed with retinoblastoma. She fought hard, survived and now has three young boys with the same diagnoses. ACCO was lucky enough to speak with the Rush family and get some insight into their unique story.
After spending four weeks in the NICU, Tristen’s parents Angie and Aaron advocated to have his eyes checked which revealed that he had retinoblastoma. “When he was diagnosed, you always hope for the best and assume everything was okay. It was really heartbreaking for us, even though my wife went through it when she was younger – it was unknown. She went through it as a baby, so when your son has it, it was kind of a whirlwind and you don’t know what to expect. It was overwhelming and heartbreaking and for a brief moment you have sadness and crying and then it turns into determination” said Aaron. Their son Caison was diagnosed at just two days old after the parents urged doctors to check his eyes after Tristen’s diagnoses. For the first six months, Carter was tumor free but in January of 2020, doctors found several tumors in his eyes. “We thought he was free and clear and that he wouldn’t have it – but we just pushed through the sadness to tackle this cancer,” said Aaron.
Each of the boys’ treatment plans have been very similar. They have all had monthly eye exams, chemotherapy for six months, laser surgery as needed and evaluations under anesthesia. The chemotherapy has caused minor hearing loss in Tristen so he wears hearing aids. Caison currently has a small vision deficit in one eye which doesn’t seem to slow him down.
 According to Aaron, the boys have been minimally affected by their diagnoses. Tristen is currently in survivors clinic status and has once a year eye exams. He is extremely personable and loves to make people laugh. He is funny, smart and full of energy. He loves to draw, playing outside, playing sports, helping around the house and swim, among other hobbies. Caison is in observation status and gets eye exams every three to four months. He is very friendly but shy. He loves to show people new things, playing in the dirt, being outside and making up funny stories. Carter is currently on active chemotherapy treatments and has monthly eye exams. He is a happy baby who smiles at everyone! He can roll over, sit up and is working on crawling.
According to Aaron, the boys have been minimally affected by their diagnoses. Tristen is currently in survivors clinic status and has once a year eye exams. He is extremely personable and loves to make people laugh. He is funny, smart and full of energy. He loves to draw, playing outside, playing sports, helping around the house and swim, among other hobbies. Caison is in observation status and gets eye exams every three to four months. He is very friendly but shy. He loves to show people new things, playing in the dirt, being outside and making up funny stories. Carter is currently on active chemotherapy treatments and has monthly eye exams. He is a happy baby who smiles at everyone! He can roll over, sit up and is working on crawling.
Please help ACCO send well wishes to the Rush family!
To learn more about retinoblastoma, please visit: https://www.acco.org/retinoblastoma/
To nominate your Gold Ribbon Hero: https://www.acco.org/gold-ribbon-heroes/
To donate to help kids like Tristen, Caison and Carter, please visit: https://www.acco.org/donate/

 Molly is an advocate for childhood cancer and has made some very exciting public appearances. She sang in front of 20,000 people at the Hockey Fights Cancer Night at the Blue Jackets and raised awareness at the Governor’s Mansion. In addition, she helps to raise awareness for pediatric cancer research by committing to ride a bike for 100 miles with her sisters.
Molly is an advocate for childhood cancer and has made some very exciting public appearances. She sang in front of 20,000 people at the Hockey Fights Cancer Night at the Blue Jackets and raised awareness at the Governor’s Mansion. In addition, she helps to raise awareness for pediatric cancer research by committing to ride a bike for 100 miles with her sisters.







 Meet Adrian, a shark and travel enthusiast that was diagnosed with Pituitary Germinoma at the age of 16.
Meet Adrian, a shark and travel enthusiast that was diagnosed with Pituitary Germinoma at the age of 16. 

